
As the New South Wales Government proposes to put more public hospitals into private control, claiming superior performance of the private sector, patients and taxpayers are entitled to ask if these privatised hospitals stack up. However, if we look at performance data today, it is not possible to make any claims they provide more effective or efficient services than publicly run hospitals.
Privately run public hospitals are becoming a more popular choice for governments, but are operating below the radar. They avoid reporting publicly on a range of performance indicators that are required for publicly run facilities. Patients and taxpayers are in the dark as to how public funds are being spent, and whether the care provided is up to standard. If the government proceeds with more privatisations, they must require that these hospitals are subject to the same performance requirements as their public hospital peers.
Privatising public hospital services
Private sector involvement in providing public healthcare is not new. In recent decades, public private partnerships (PPP) in health have become more popular with governments of all persuasions. Across the country a number of PPPs have been developed whereby a private provider takes responsibility for building and operating a new public hospital.[1] Some of these PPP arrangements, including the Casey Hospital and Port Macquarie Hospital PPPs, have been found to have a mixed record in providing value for money and quality for taxpayers.[i]
These arrangements build on discussion over many years of the merits of inviting the private sector to deliver more public services. The current Commonwealth Government has actively advocated for privatisation,[ii] and the Productivity Commission last year recommended more “contestable approaches to commissioning services”.[iii] The Centre for Independent Studies (CIS) has called for greater involvement of the private sector to “encourage productivity and improve access to quality hospitals services at the least cost”.[iv] In 2013 the Queensland Government announced that the new Sunshine Coast University Hospital will be built and operated by a private provider,[v] with the Queensland Health Minister highlighting the benefits from such an approach. Most recently, the NSW Government likewise announced it will establish the new Northern Beaches Hospital under this model, and is currently inviting the private sector to do so at five public facilities in the state.[vi] Premier Baird claimed such a model will provide an opportunity to give patients “the best possible services for NSW we can get,” and that it would “maintain quality healthcare while delivering the best value”.
These statements ignore comprehensive non-partisan evaluations that have failed to show private hospitals outperform public hospitals.[vii] Rather, they appear to be based on a belief or an “ideological commitment”[viii] that the private sector delivers higher quality services more efficiently than the public sector.[ix]
This is a familiar ideological debate between the defenders of public (government) managed services and those favouring a stronger role for the private sector.
Despite the long held debate, little attention has been paid to how these hospitals actually perform under privatised arrangements. With a number of privatisations planned, we need to look closely at whether privately operated public hospitals are delivering better value services for the taxpayer, as claimed.
To do this, an objective analysis was done on performance of the small number of health facilities that are publicly funded and privately delivered (“privatised” for the purpose of this paper) and ask the question: do privatised hospitals outperform their publicly run peers? Is the rhetoric from politicians matched by actual performance?
Note that the relative merits of public and private health service delivery, or the pros and cons of PPPs were not examined in this paper – though those debates and analyses are ongoing.[x]
The current performance reporting system
Public and private hospitals both have an important role in the health of the communities they serve. Australians are deeply invested in ensuring their local hospital is adequately resourced and performing well. Thanks to policy changes to improve transparency in recent years, the community is regularly informed about how their local public hospital is performing against national benchmarks and compared to other hospitals.
Australia’s hospitals spent more than $69 billion of recurrent expenditure in 2014-15, and about 90 per cent of care in public hospitals and 32 per cent of care in private hospitals is funded by Australia’s taxpayers.[xi]
This is an enormous investment of Australia’s resources. The 2011 COAG National Health Reform Agreement reflected a growing recognition of the need for transparency, accountability and performance reporting.[xii] The Agreement introduced a Performance and Accountability Framework for nationally consistent information on the performance of all health and hospital services, including private hospitals.[xiii]
Importantly, the Agreement includes a provision to cover ‘private or not for profit provision of public hospital services’ in which hospitals covered by these arrangements are treated as a public hospital for the purpose of the Agreement.[xiv] Under this reporting system, public and private hospitals are now required to publicly report on a range of clinical and financial outcome performance metrics,[xv] through the My Hospitals website run by the Australian Institute of Health and Welfare (AIHW).
In addition, given the large sums of taxpayer funding invested in their operation, public hospitals are also subject to close parliamentary scrutiny. As a result, the public are generally well informed about the quality and financial performance of their local public hospitals. Private hospitals are formally included in the reporting framework and required to provide data to the AIHW for analysis and publishing on My Hospitals.
Defining “privatised hospitals”
There is no accepted definition of privatised hospitals, and My Hospitals isn’t clear on which funding model applies to the hospitals reported. For our purposes, and borrowing a similar definition from the CIS, the following definition was used to identify privatised hospitals:
- The hospital is not operated by a state or territory health department or health district; and
- The hospital is not owned or operated by a faith- based or not-for-profit health provider; and
- The hospital is owned by the state but operated by a private, for-profit provider and funded by the state to provide public services; or
- The hospital is owned and operated by a private, for-profit provider and funded by the state to provide public services.
Drawing on the My Hospitals website and publicly available information from government and private operators’ websites, there are currently five hospitals in Australia that meet these criteria:
- Joondalup Health Campus, WA (classified as a major metropolitan hospital by My Hospitals);
- Peel Health Campus, WA (a large metropolitan hospital);
- Mildura Hospital, VIC (a large regional hospital);
- Noosa Hospital, QLD (unclassified); and
- Sunshine Coast University Hospital, QLD (unclassified).
All five hospitals are operated by Ramsay Healthcare, a publicly listed multi-national company which operates 70 health facilities around Australia and many others internationally.[xvi]
Although a small number of facilities to examine, some useful comparisons can be made and to demonstrate where comparable performance data aren’t available.
All performance data has been drawn from publicly available sources, in particular the My Hospitals website and the state health department performance websites. To enable a fair evaluation of performance, the five facilities will be compared, where possible, against the performance of their “peer” public hospitals.[2]
The My Hospitals website lists individual hospital performance against a number of metrics. A selection of performance metrics has been selected for this comparison, including access, clinical performance, safety and quality and financial measures:
- Emergency department waiting times for triages 3, 4 and 5;
- Emergency department ‘four hour rule’;
- Average length of stay for selected medical conditions and surgical procedures: childbirth, Chronic Obstructive Pulmonary Disease (COPD), heart failure, knee replacement, hysterectomy, prostate removal;
- Healthcare acquired infections and hand hygiene compliance (a proxy for patient safety); and
- Average cost per procedure (a proxy for financial performance).
How do they stack up?
Taking these five measures, we look at how the five privatised hospitals compare to their peers:
- Emergency Department triage waiting times (green indicates better than peer performance, red worse than peer performance)
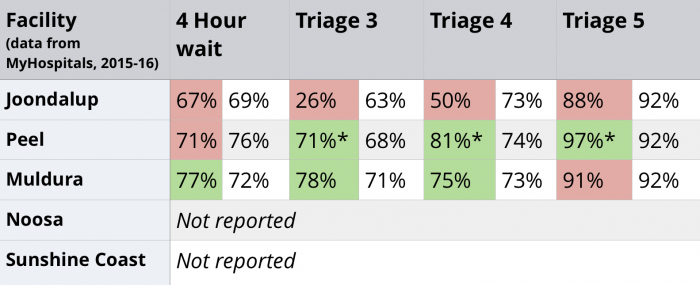
*Data is from 2013-14, the latest data available on My Hospitals. Data for the past two financial years for Peel is unavailable on either MyHospitals or the WA Health website.
Overall, performance was mixed, with two of the three reporting hospitals outperforming their peers in a majority of categories. However, Joondalup Hospital had longer wait times than its peer hospitals for all triage and wait categories. It should be noted that Peel’s data is older due to a lack of updated publicly available data. More up to date data was requested from WA Health but not received. Neither of the Queensland hospitals report any emergency department performance data publicly.
- Length of stay (LOS) selected medical conditions
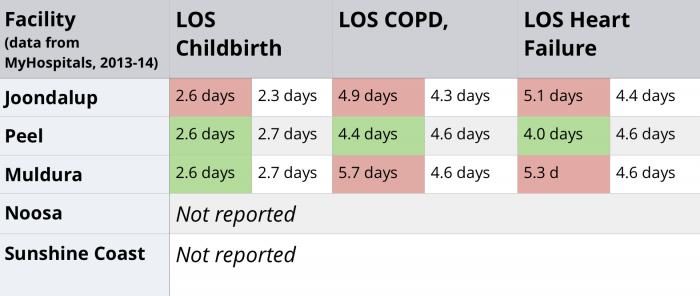
Again, performance was mixed, with a slight underperformance in the data. Joondalup had longer stays in all of the selected categories. Peel Hospital performed better than its peers in all three categories, whilst Mildura had longer waits in two of the three categories. Neither of the Queensland hospitals publicly reported on any medical condition performance.
- Length of stay (LOS) surgical procedures
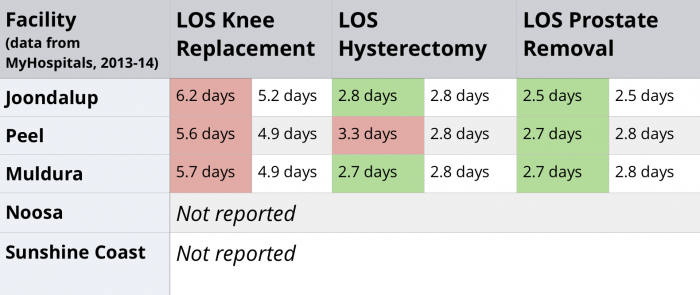
On this measure, Joondalup, Peel and Mildura all performed worse than their peers with length of stay for knee replacements. However, all three outperformed their peers with length of stay for prostate removals. Results for hysterectomy length of stay were mixed. Again, neither of the Queensland hospitals report any performance data.
- Safety and quality
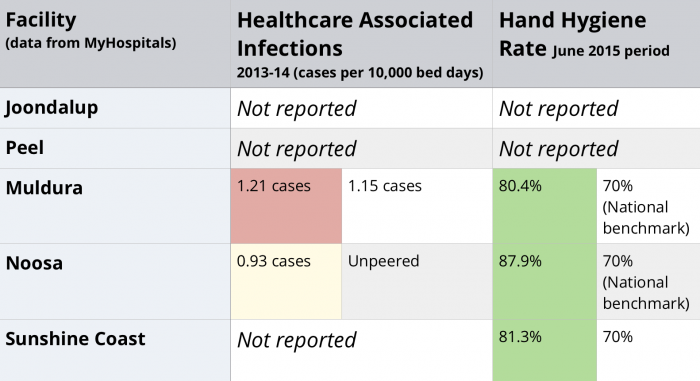
On the two measures for safety and quality, there is a concerning lack of data. Neither of the West Australian hospitals have data on My Hospitals or the WA Health website. Mildura Hospital performed better than the national benchmark for hand hygiene, but below its peers on healthcare associated infections. Hand Hygiene compliance had the only reported data on My Hospitals for the two Queensland Hospitals, with Noosa and Sunshine Coast hospitals both exceeding the national benchmark for hand hygiene rates. Noosa’s healthcare acquired infection rate of 0.93 cases is unpeered, precluding a comparison, whilst Sunshine Coast did not report on this measure.
- Financial performance
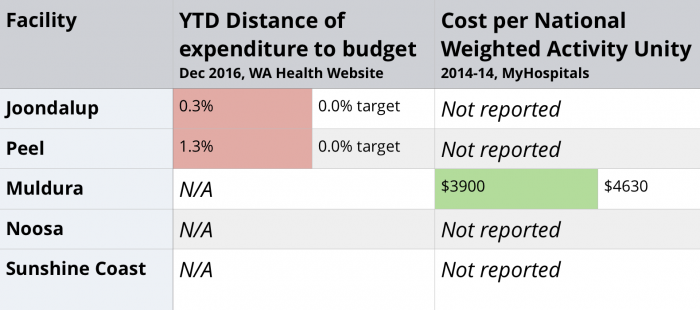
The only hospital that had financial data on My Hospitals was for Mildura. Mildura had a National Weighted Activity Unit cost significantly lower than its peers in 2013-14, indicating that Mildura is delivering services more efficiently than its peers.
From the latest data available on the WA Health website, Joondalup and Peel are both exceeding their budget. These data do not provide any detail on the amount of the budget overspend, nor allow for a comparison with peer hospitals, so there are clear limitations to this data.
Neither of the two Queensland hospitals report any financial data on the My Hospitals or Queensland Health websites.
Findings – where is the evidence?
A close look at the available performance information on these hospitals highlights two key issues:
- There are significant gaps in performance data for privatised hospitals. Despite the Health Reform Agreement requiring all hospitals to submit performance data to My Hospitals,[xvii] the information is incomplete and often incomparable. Public hospitals provide much more performance data on clinical, access and financial performance compared to private and privatised hospitals. Many private hospitals do not have an emergency department, and so less data on private hospital access performance, and private hospitals can claim commercial in confidence exemptions from reporting on financial performance.
The five privatised hospitals have a very mixed record in reporting. Whilst Joondalup, Peel and Mildura have data on most clinical and access indicators, there is almost a complete absence of performance data for the two Queensland hospitals. This is a significant gap in financial performance reporting and on the safety and quality measures, which is a concerning lack of transparency in the expenditure of taxpayer funds and achievement of quality standards.
- Based on the limited data available, it is not possible to make an informed decision on the performance of privatised hospitals. The data that are reported, mainly by Joondalup, Peel and Mildura hospitals, show that performance in emergency department waiting times and lengths of stay for surgical and medical procedures are mixed.
The privatised hospitals perform better in some measures, and worse in others. Alarmingly, there is insufficient data to make any comparisons on safety and quality, and financial performance. It is simply not possible to make any comment on the Queensland hospitals, given the almost complete lack of performance data reported.
So, when the public rightly asks “do privatised hospitals outperform their public hospital peers?” the answer, in short, is another question: “how can we tell?” There is simply insufficient performance data reported by the privatised hospitals to allow for any considered answer to this question.
It appears that when governments invite the private sector to provide public services, the reporting and accountability arrangements are not clearly defined, or are not requiring the new operators to report on performance- or both. The lack of transparent performance reporting by these hospitals is concerning for a number of reasons:
- Spending health dollars ethically and in line with community expectations demands transparency in investments made on behalf of the public.
- Health costs will continue to increase, and Australia’s governments will come under increasing pressure to maintain or improve outcomes and finance the system. All health expenditure needs then to be transparent and assessed to ensure it is targeted to meet the health needs of the community at the lowest cost.
- The community has a large stake in the effectiveness of hospital care, and so public hospitals are rightly subject to scrutiny. As the service contracts between the state and the private provider cover many years (for example, 20 years in the case of Joondalup), the absence of performance data on publicly funded privatised hospitals therefore constitutes a “democratic deficit”,[xviii] as taxpayers and patients are unable to exercise judgement on the performance of these publicly funded services.
- The lack of reporting by the privatised hospitals also undermines the intent of the performance reporting system for all hospitals, as it works best when all providers participate.[xix] In addition to the intrinsic and ethical benefit of transparency, evidence suggests that public reporting stimulates hospital improvement activity.[xx]
- Favouring private investments while not compelling reporting undermines the requirements of the Performance and Accountability Framework signed by all governments, the approach to their public hospitals, and of course, community expectations.
As Australia’s governments prepare to begin the next round of negotiations for the next hospital funding agreement, this ambiguity should be addressed, so that all taxpayer funding for hospital services is properly accounted for and reported transparently. Publicly reporting on performance is now an expectation of all other hospitals in Australia, and bringing the privatised hospitals into the reporting framework will place the same requirements on them that are placed on their peers.
Recommendations
Recommendation 1: Bring privatised hospitals into the Performance and Accountability Framework
Whilst the National Health Reform Agreement states that privatised hospitals are to be treated as public hospitals, this provision has not carried over to the Performance and Accountability Framework that sits under the Agreement. The next hospital funding agreement signed by COAG needs to explicitly clarify how privatised hospitals are to be treated in terms of reporting and accountability.
Recommendation 2: Publish privatised hospital performance data on My Hospitals
Privatised hospitals must be required to report on their performance in the same manner as their public hospital peers through My Hospitals. This includes the same clinical, access and financial performance data that all public hospitals are required to report on. The community is entitled to expect the same accountability measures for these hospitals and to be able to make informed decisions about their performance.
Conclusion
We can see that taxpayers are not given the chance to know how privatised hospitals are performing- whether they are receiving value for money and quality care. The meagre amount of data doesn’t allow for any definitive conclusions; this fact alone tells us it is misleading to claim that the private sector delivers a superior or lower cost service. These claims simply are not based in evidence because there isn’t any. The absence of data exposes these claims as ideologically driven political rhetoric. Taxpayers and patients deserve better than that.
Footnotes
[1] For example, the Royal North Shore Hospital redevelopment was a PPP arrangement whereby the private consortium financed the reconstruction costs of the hospital and will operate non clinical services at the hospital on behalf of the government for the life of the contract.
[2] Hospitals on My Hospitals are grouped to allow for fair and meaningful comparisons with similar hospitals and minimise the effect of different hospital size, service provision mix and regional/rural location.
References
[i] McKell Institute, Risky Business: the pitfalls and missteps of hospital privatisation, November 2014, accessed on 15 December 2016 at https://www.hsu.asn.au/wp-content/uploads/2015/02/McKell_Hospitals_A4_V3.pdf
[ii] Australian Government, Australian Treasury, National Commission of Audit final report, March 2014, accessed on 15 December 2016 at http://www.ncoa.gov.au/report/index.html
[iii] Productivity Commission, Study Report: Introducing completion and informed user choice into human services: identifying sectors for reform, November 2016, accessed on 22 December 2016 at http://www.pc.gov.au/inquiries/current/human-services/identifying-reform/report
[iv] Gadiel D, Sammut J, ‘How the NSW Coalition should govern health: strategies for microeconomic reform’, 2012, Centre for Independent Studies, accessed on 15 December 2016 at https://www.cis.org.au/product/how-the-nsw-coalition-should-govern-health-strategies-for-microeconomic-reform
[v] Guest A, ABC News, Queensland Government to privatise new $1.8 billion Sunshine Coast University Hospital, 25 July 2013, accessed on 20 February 2017 at http://www.abc.net.au/news/2013-07-25/qld-government-to-privatise-new-sunshine-coast-public-hos/4842242
[vi] Robertson J, Sydney Morning Herald, Five NSW Hospitals to be privatized under surprise plan, 9 September 2016, accessed on 20 February 2017 at http://www.smh.com.au/nsw/five-nsw-hospitals-to-be-privatised-under-surprise-plan-20160915-grh6mq.html
[vii] Productivity Commission, Research Report: Public and Private Hospitals, December 2009, accessed on 28 December 2016 at http://www.pc.gov.au/inquiries/completed/hospitals/report
[viii] Corderoy, A, The Guardian, Our hospitals are being privatized. Is anyone paying attention?, 20 September 2016, accessed on 7 January 2017 at https://www.theguardian.com/commentisfree/2016/sep/20/our-hospitals-are-being-privatised-is-anybody-paying-attention
[ix] Quiggin J, op. cit.
[x] See McKell 2014, Productivity Commission 2009, Commission of Audit 2014, op. cit.
[xi] Australian Institute of Health and Welfare, Australian hospital statistics 2014-15, 2015, accessed on 19 January 2017 at http://www.aihw.gov.au/WorkArea/DownloadAsset.aspx?id=60129555677
[xii] Council of Australian Governments, National Health Reform Agreement, 2011, p.44, accessed on 3 February 2017 at http://www.federalfinancialrelations.gov.au/content/npa/health/_archive/national-agreement.pdf
[xiii] Australian Institute of Health and Welfare, National Health Reform Performance and Accountability Framework, 2011, p.4, accessed on 3 February 2017 at http://www.aihw.gov.au/WorkArea/DownloadAsset.aspx?id=60129555677
[xiv] National Health Reform Agreement, op.cit, p.20
[xv] National Health Reform, Performance and Accountability Framework, op.cit.
[xvi] Ramsey Health Care, www.ramseyhealth.com.au,
[xvii] National Health Reform Agreement, op.cit., p.44
[xviii] Duckett S, Grattan Institute, Public-private partnerships are risky business, 30 July 2013, accessed on 31 January 2017 at https://grattan.edu.au/news/public-private-hospital-partnerships-are-risky-business/
[xix] Leape LL, Transparency and Public Reporting Are Essential for a Safe Health Care System, March 2010, The Commonwealth Fund, accessed on 20 January 2017 at http://www.commonwealthfund.org/publications/perspectives-on-health-reform-briefs/2010/mar/transparency-and-public-reporting-are-essential-for-a-safe-health-care-system
[xx] Fung CH, Lim Y, Mattke S, Damberg C, Shekelle PG, Systematic Review: The evidence that publishing patient care performance data improves quality of care, 2008, Ann Intern Med, 148:111-123

SOCIAL SHARE